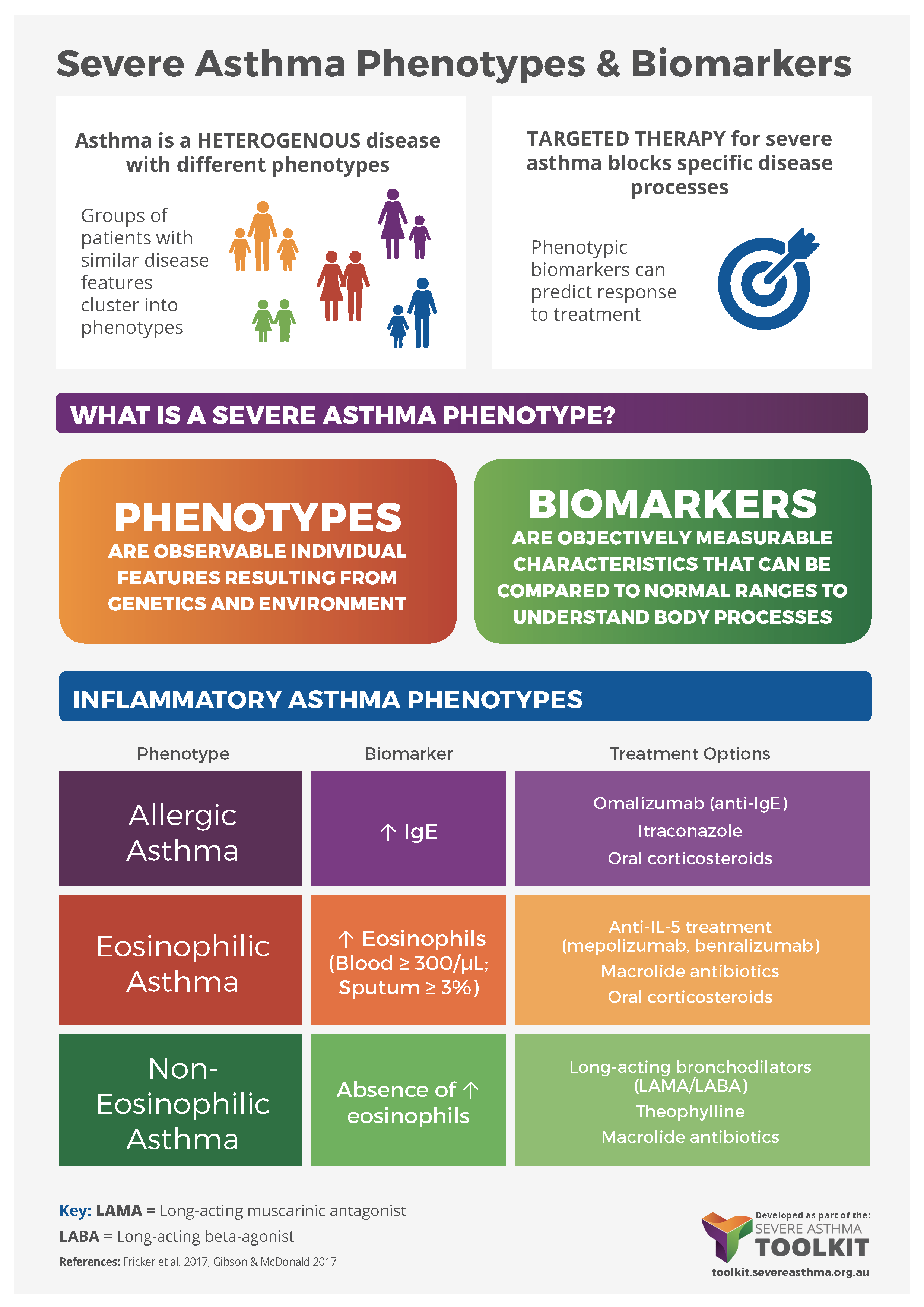
Asthma is a heterogeneous disease, with individual patients presenting with different symptoms, pathology and underlying disease mechanisms, termed “phenotypes”.
It is increasingly important to identify individual phenotypes to inform diagnosis and disease management. This is particularly critical for targeted therapies, which reduce a patient’s symptoms by blocking very specific disease pathways. Targeted therapies are only effective in patient subgroups where those specific pathways are actually responsible for disease. For example, omalizumab monoclonal antibody therapy targets IgE and mepolizumab targets IL-5. For more information see Medications – Monoclonal Antibodies